Age- and Sex-Associated Impacts of Body Mass Index on Stroke Type Risk: A 27-Year Prospective Cohort Study in a Low-Income Population in China
 Hongfei Gu1†,
Hongfei Gu1†,  Shuang Shao2†, Jie Liu3,4,5,
Shuang Shao2†, Jie Liu3,4,5,  Zhenqian Fan2,
Zhenqian Fan2,  Yu Chen2, Jingxian Ni3,4,5, Conglin Wang6, Jun Tu3,4,5,
Yu Chen2, Jingxian Ni3,4,5, Conglin Wang6, Jun Tu3,4,5,  Xianjia Ning3,4,5, Yongzhong Lou1*, Bin Li1* and
Xianjia Ning3,4,5, Yongzhong Lou1*, Bin Li1* and  Jinghua Wang3,4,5*
Jinghua Wang3,4,5*- 1Department of Neurology, Tianjin Haibin People's Hospital, Tianjin, China
- 2Department of Endocrinology and Metabolism, The Second Hospital of Tianjin Medical University, Tianjin, China
- 3Department of Neurology, Tianjin Medical University General Hospital, Tianjin, China
- 4Laboratory of Epidemiology, Tianjin Neurological Institute, Tianjin, China
- 5Key Laboratory of Post-Neuroinjury Neuro-Repair and Regeneration in Central Nervous System, Tianjin Neurological Institute, Ministry of Education, Tianjin, China
- 6Department of Geriatrics, Tianjin Medical University General Hospital, Tianjin, China
The relationship between body mass index (BMI) and stroke type has remained controversial despite studies demonstrating that BMI is related to stroke risk, especially in specific groups. We assessed the age- and sex-associated impacts of BMI on stroke type in a low-income, poorly educated population in China. The association of BMI with stroke type was estimated using Cox regression analyses in this prospective cohort study, after adjusting for sex, age, education level, hypertension, diabetes, smoking, and alcohol drinking status. During the follow-up period, 638 stroke cases occurred among the 3,906 participants included in this prospective study. For men aged <65 years, being overweight was an independent predictor of all stroke subtypes, compared with normal-weight individuals; the hazard ratios (HRs) and 95% confidence intervals (CIs) were 1.98 (1.52–2.58) for total stroke, 1.69 (1.22–2.33) for ischemic stroke, and 3.62 (2.09–6.25) for hemorrhagic stroke, all P < 0.001. Being underweight was also an independent predictor of hemorrhagic stroke (HR, 5.10; 95%CI, 1.80–14.50, P = 0.002). For women <65-years-old, being overweight was a risk factor for total (HR, 1.38; 95% CI, 1.01–1.89; P = 0.044) and hemorrhagic strokes (HR, 2.06; 95% CI, 1.00–4.28; P = 0.050); obesity was a risk factor for total (HR, 2.47; 95% CI, 1.60–3.82) and ischemic strokes (HR, 2.53; 95% CI, 1.54–4.15), all P < 0.001. These findings suggest that weight management should be a high priority for substantially reducing the heavy burden of strokes in rural China among both men and women <65-years-old; men<65-years-old should maintain their weight within a reasonable range.
Introduction
Stroke has recently become the leading cause of death in China (1), accounting for almost one-third of the total number of stroke-related deaths, worldwide (2). In 2013, 27 of China's 33 provinces reported strokes as the main cause of death (3). The proportion of adults with a body mass index (BMI) ≥25 kg/m2 increased globally between 1980 and 2013, among both men (from 28.8 to 36.9%) and women (from 29.8 to 38.0%) (4).
The positive association between BMI and ischemic stroke is well-established (5–8). For hemorrhagic stroke, the results of previous studies have been more disparate, with some reports showing a linear, positive correlation (6, 7, 9–11) with BMI, others showing a J-shaped or U-shaped relationship (9, 12, 13), and some showing no correlation (14, 15) or a linearly opposite correlation (16). Such discrepancies may be due to differences in the risk factors and stroke incidences among different populations.
In low- and middle-income countries, 22.4% of the stroke burden (measured using disability-adjusted life years) is attributable to high BMIs; separate estimates for pathological types and patient age and sex were not reported (17). Moreover, our previous study revealed the increased burden of stroke in young and middle-aged adults (18). Thus, we aimed to assess the age-and sex associated relationship between BMI and total, ischemic, and hemorrhagic strokes, in a rural population in Tianjin China.
Methods
Study Population and Sample Process
The study cohort was derived from a population-based stroke monitoring study. The baseline investigation was performed in October 1991, and stroke events were recorded until to February 2018. The study population was previously described (18–21). Briefly, it included 14,936 people (in 1991), 95% of whom were low-income farmers living in 18 administrative villages. The main source of income for the residents was cereal crop production, with annual per capita incomes of <100 USD in 1990 and <1,000 USD in 2010 (22).
The sampling method used in this cohort study was also previously reported (23). Briefly, all residents within the 18 administrative villages in the region were recruited into the study. The villages were divided into three geographic regions (east, south, and north) and two villages from each region were randomly selected. Using a stratified cluster sampling approach, we selected all residents who were from the six villages, aged ≥15 years, and without evidence of coronary heart disease or stroke to participate in the study. For the purposes of this analysis, only participants aged ≥18 years were included.
The investigative protocol was approved by the ethics committee of Tianjin Medical University General Hospital, and a written informed consent was obtained from each participant.
Baseline Information
Demographic characteristics (including sex, age, and educational level), past medical history (including hypertension, diabetes, stroke, and cardiovascular disease), and personal lifestyle (including smoking habits and alcohol consumption) were recorded, and these were from self-reported by participants. All information was collected in face-to-face interviews by trained local researchers conducting. Physical examinations, including blood pressure (BP), height, and weight measurements, were also conducted during the interviews.
Measurement Methods and Definition
BP was measured in the supine position using methods described previously (23). Height and weight were measured using a height and weight meter with the participants in light clothing. Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m).
Hypertension was defined as a self-reported previous hypertension history, or use of antihypertensive medicine, or SBP/DBP of 140/90 mmHg at baseline; diabetes was defined as a self-reported previous disease history or current use of antidiabetics. Underweight was defined as a BMI<18 kg/m2, normal weight as a BMI of 18–23.9 kg/m2, overweight as a BMI of 24–27.9 kg/m2, and obesity as a BMI ≥28 kg/m2 (24).
Case Definition
We previously published the stroke monitoring and protocol details used to diagnose stroke and determine stroke types (18–21). Stroke was defined as a first-ever, acute, focal, neurological deficit of vascular etiology that lasted >24 h.
All first-ever stroke events were diagnosed as full clinical stroke, with obvious clinical signs and symptoms. Stroke events including hemorrhagic, ischemic, and undetermined strokes, were diagnosed by neuroimaging within 72 h of stroke onset. Hemorrhagic stroke was defined as an intracerebral hemorrhage (ICH) or subarachnoid hemorrhage. Ischemic stroke (IS) was defined as a thrombotic brain infarction, cardioembolic stroke, or lacunar infarct. Undetermined stroke was defined as stroke that could not be classified into the previously described types because there was absence the neuroimaging evidence; but all these patients were symptomatic stroke.
In this study, subarachnoid hemorrhage, transient ischemic attacks (TIAs) and silent strokes (diagnosed via imaging, only) were excluded. Patients with transient symptoms but with neuroimaging evidence of cerebral infarctions were considered stroke cases (25). Moreover, those patients caused by other causes with stroke-relative symptom were excluded in this study.
Subgroup analysis of stroke types in this study was included IS, ICH, and stroke (included IS, ICH, and undetermined stroke) to assess the association of BMI with stroke risk.
Stroke Event Ascertainment and Processes
The stroke case ascertainment process was as described previously (18). Briefly, stroke events were reported according to predefined procedures. First, a local licensed village doctor reported stroke events to physicians in the community hospital within 24 h of patient presentation. Second, community hospital physicians visited surviving patients within 72 h to obtain clinical feature information and confirm the occurrence of stroke. Each month, these physicians reported confirmed stroke events (diagnosed by imaging) to Tianjin Medical University General Hospital (TMUGH); suspected events (no imaging performed) were also reported in a timely manner. Finally, as soon as possible, a TMUGH neurologist identified suspected cases during door-to-door interviews.
The community hospital physicians and TMUGH neurologist collected information regarding stroke onset during interviews with the patient or patient's family. The collected information included patient demographics, time of stroke onset, clinical signs, and previous stroke status. The TMUGH neurologist also obtained other information, including therapy and post-discharge outcomes, the during interviews with the surviving patients or their family members.
Statistical Analysis
Continuous variables (age, BP, and BMI) are expressed as means (standard deviations) and categorical variables are expressed as 95% confidence intervals (CIs). Age-standardized incidences were calculated using the direct method of world standard population age groupings: <45, 45–64, and ≥65 years (26). Subgroup analyses were conducted to evaluate the risk of first-ever stroke by age (<65 years, and ≥65 years), educational attainment (illiterate, 1–6 years of schooling, and >7 years of schooling), BMI group (underweight, normal, overweight, obese), smoking status (never smoked, ever smoked, and current smoking), and alcohol consumption status (never drank, ever drank, and current drinking). Association of BMI with the risk of developing stroke was assessed by Kaplan-Meier survival analysis and presented as a survival curve. We estimated the hazard ratio (HR) of BMI on stroke, with and without adjusting for sex, age, education level, hypertension, diabetes, smoking, and alcohol drinking status, using Cox regression analyses. The follow-up time (recorded in years) was calculated as the interval between the date at baseline and the date of the occurring stroke for patients experiencing a first-ever stroke during the study period. For participants without further stroke events, the follow-up time was defined as 26.3 years. Moreover, for participants who died during the study periods, the follow-up time was defined as the interval between baseline and the date of death. Data for patients who were lost to follow-up or who emigrating were censored. All statistical analyses were performed using SPSS for Windows (version15.0; SPSS, Chicago, IL, USA); P-values < 0.05 were considered statistically significant.
Results
Participant Characteristics
During the 27 years of follow-up, a total of 638 strokes occurred among the 3,906 participants, including 404 ischemic, 121 hemorrhagic, and 113 undefined strokes. The cumulated incidence of stroke in this population was 16.3% overall.
The 3,906 individuals involved in the study had an average age of 41.74 years and included 1,834 men (47.0%) and 2,072 women (53.0%); 40.7% of the participants had never received any formal education (men, 36.8%; women, 44.1%). The prevalence of hypertension and diabetes at baseline was 31.0 and 0.1%, respectively; the percentages of participants who were current smokers and alcohol consumers were 25.7 and 15.4%, respectively. The average BMI for these individuals was 22.58 kg/m2 at baseline (Table 1).
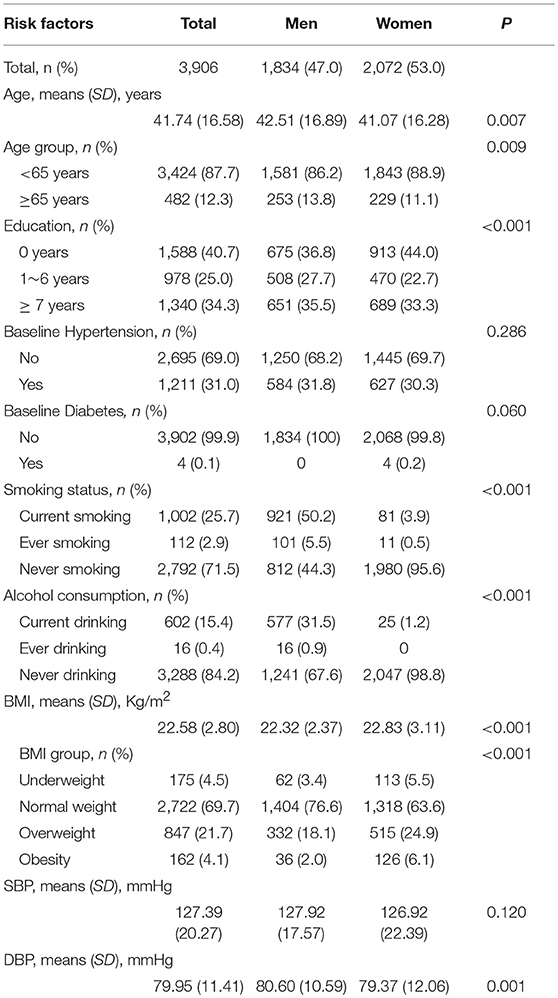
Table 1. Demographic characteristics and risk factors of all participants in this study.
Distribution of Stroke Risk Factors in This Population at Baseline by BMI
The prevalence of overweight and obesity was much higher among women than among men (24.9 vs. 18.1%, and 6.1 vs. 2.0%, respectively; P < 0.001). In this population, participants with hypertension tended to have higher rates of being overweight or obese than those without hypertension, with the corresponding rates of overweight and obesity being 28.5 vs. 18.6%, and 7.3 vs. 2.7%, respectively; P < 0.001 (Table 2).
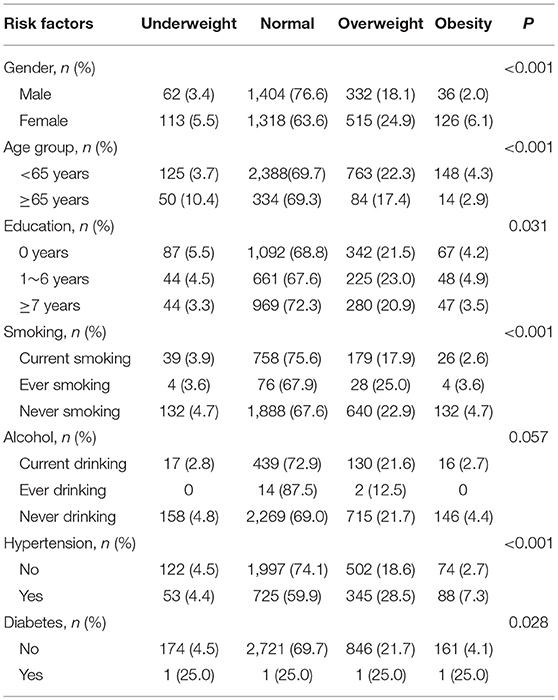
Table 2. Distribution of stroke risk factors in this population at baseline by BMI.
Association of BMI With Total, Ischemic, and Hemorrhagic Stroke in Kaplan-Meier Survival Analysis
Figure 1 shows that BMI is associated with occurrence of a first-ever stroke overall, all P < 0.001. The highest survival rate was observed among patients with obesity at baseline across all stroke types. Similar results were found in patients aged <65 years. However, a significant association was not found in elderly patients aged 65 years and older.
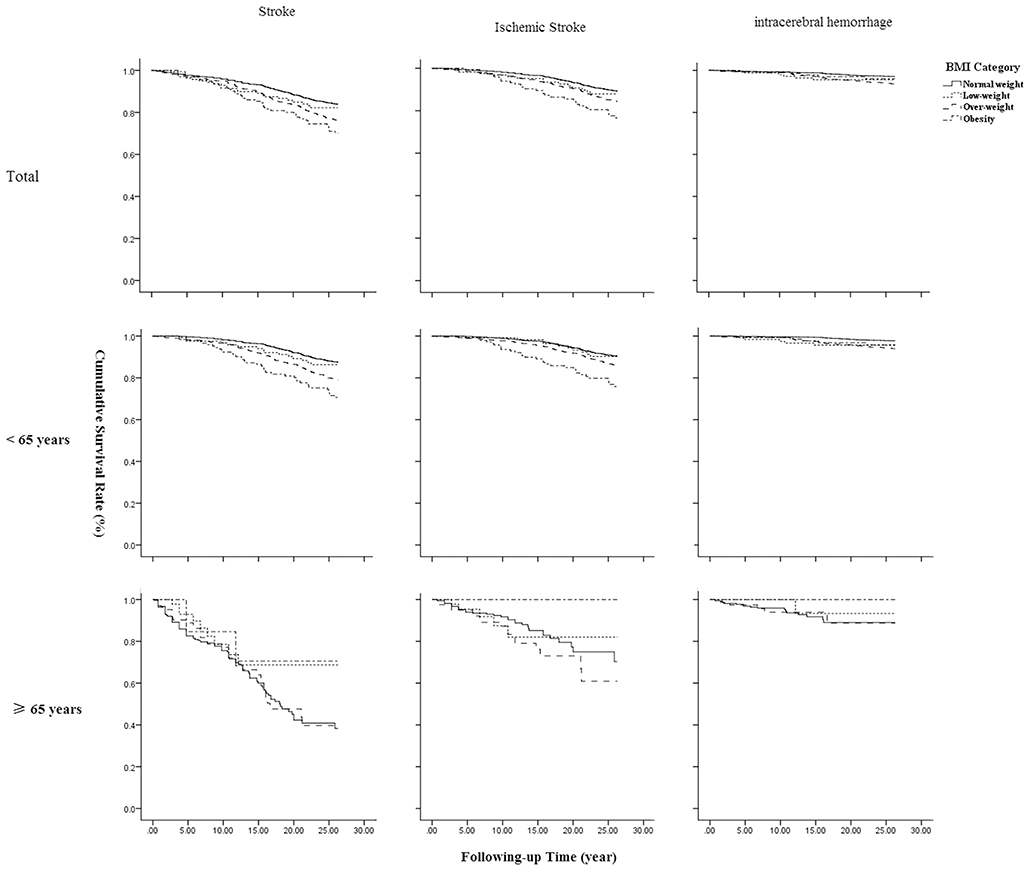
Figure 1. Association of BMI with stroke survival by types and age.
Association of BMI With Total, Ischemic, and Hemorrhagic Stroke Using Cox Regression Analysis
Compared with patients of normal baseline weights, the HRs (95% CIs) associated with being overweight at baseline were 1.48 (1.24–1.77; P < 0.001) for total stroke, 1.43 (1.14–1.80; P = 0.002) for ischemic stroke, and 2.34 (1.58–3.47; P < 0.001) for hemorrhagic stroke, after adjusting for confounders. Obesity at baseline was significantly and positively associated with both total and ischemic stroke, with HRs (95% CIs) compared to normal-weight individuals, of 2.00 (1.44–2.79) for total stroke and 2.16 (1.46–3.21) for ischemic stroke, respectively, all P < 0.001. There was no statistically significant association between being underweight at baseline and stroke (Table 3; Figure 2).
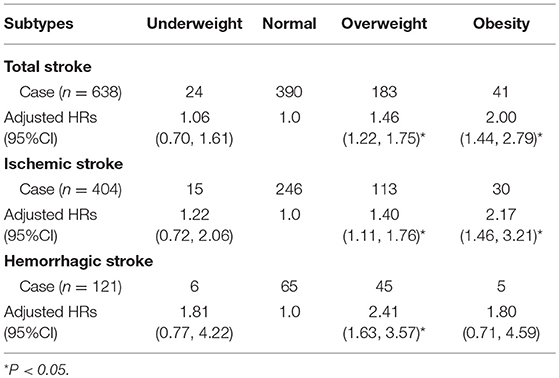
Table 3. Association of BMI with total, ischemic, and hemorrhagic stroke using Cox regression analysis.
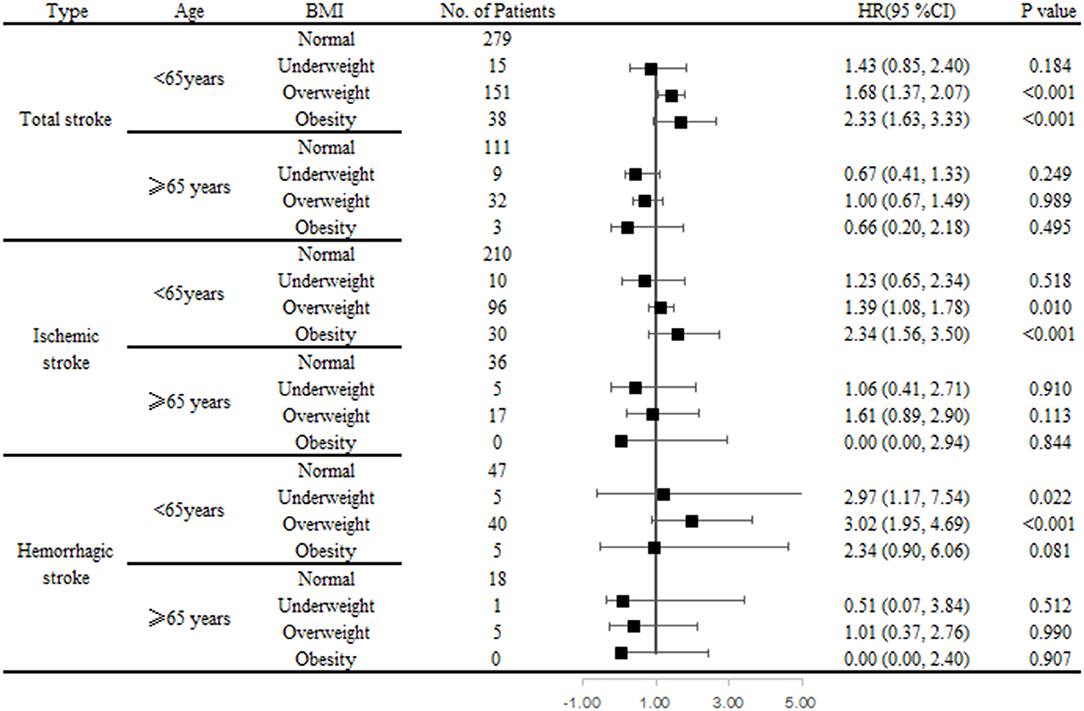
Figure 2. Association of BMI and stroke risk by types and age groups using Cox regression analysis.
Association of BMI With Total, Ischemic, and Hemorrhagic Stroke by Age Using Cox Regression Analysis
Among individuals aged <65 years, being overweight was an independent determinant of stroke, regardless of stroke type, compared with normal weight individuals; the HRs (95% CIs) were 1.69 (1.38–2.07; P < 0.001) for total stroke, 1.42 (1.11–1.81; P = 0.006) for ischemic stroke, and 2.93 (1.88–4.56; P < 0.001) for hemorrhagic stroke. Obesity was significantly associated with developing both total (HR, 2.35; 95% CI, 1.65–3.36; P < 0.001) and ischemic (HR, 2.35; 95% CI, 1.57–3.51; P < 0.001) strokes. Being underweight was also associated with hemorrhagic stroke risk (HR, 3.18; 95% CI, 1.26–8.05; P = 0.002). However, among individuals aged ≥65 years, there was no correlation between BMI and stroke, regardless of type (Table 4).
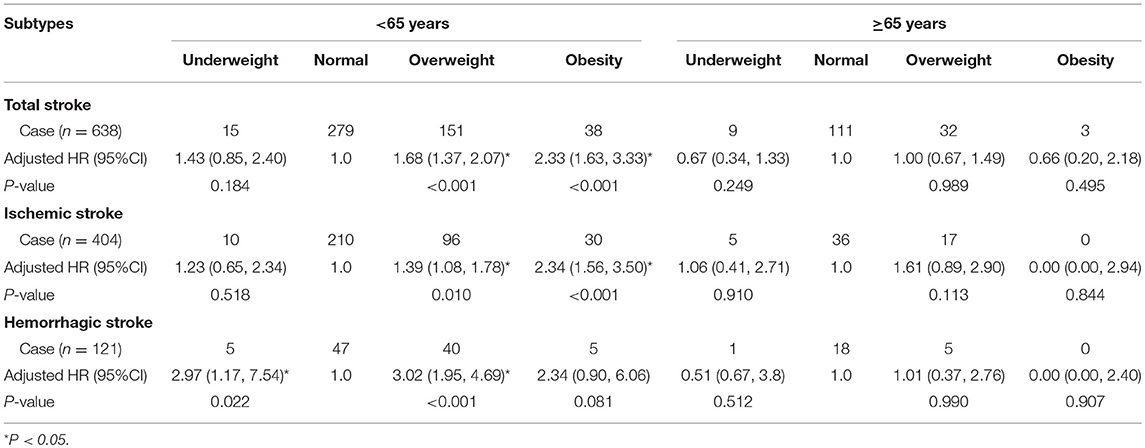
Table 4. Association of BMI with total, ischemic, and hemorrhagic stroke by age using Cox regression analysis.
Association of BMI With Total, Ischemic, and Hemorrhagic Stroke Using Cox Regression Analysis Among Population Aged <65 Years
For men aged <65 years, being overweight was an independent determinant of all stroke types, relative to normal weight individuals; the HRs (95% CIs) were 1.98 (1.52–2.58) for total stroke, 1.69 (1.22–2.33) for ischemic stroke, and 3.62 (2.09–6.25) for hemorrhagic stroke (all P < 0.001). Importantly, being underweight was also an independent determinant of hemorrhagic stroke (HR, 5.10; 95%CI, 1.80–14.50, P = 0.002). However, there was no relationship between obesity and any stroke type.
For women aged <65 years, compared with normal weight individuals, being overweight was a risk factor for total (HR, 1.38; 95% CI, 1.01–1.89, P = 0.044) and hemorrhagic (HR, 2.06; 95% CI, 1.00–4.28, P = 0.050) strokes; obesity was a risk factor for total (HR, 2.47; 95% CI, 1.60–3.82) and ischemic (HR, 2.53; 95%CI, 1.54–4.15) stroke, all P < 0.001; being underweight was not associated with any stroke type (Table 5).
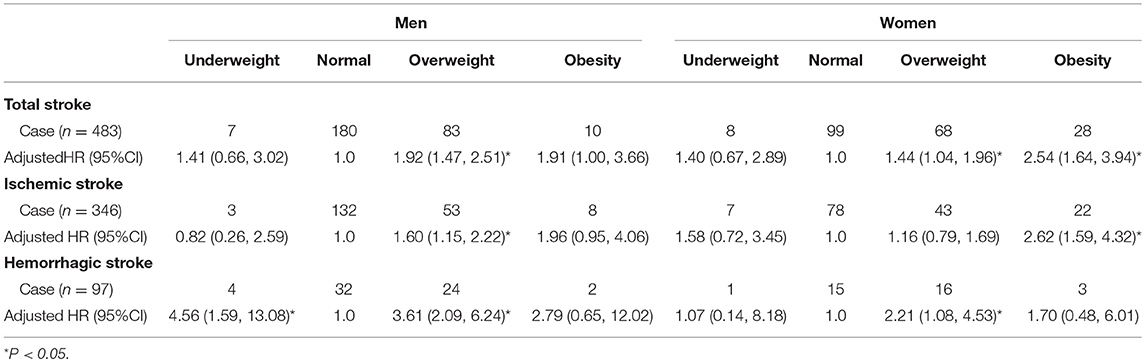
Table 5. Association of BMI with total, ischemic, and hemorrhagic stroke using Cox regression analysis among population aged <65 years.
Discussion
In this large, prospective, cohort study of 3906 persons with 27 years of follow-up, we evaluated the age- and sex-associated correlations of BMI with the risk of total, ischemic, and hemorrhagic strokes. Overall, being overweight at baseline increased the risk of both ischemic and hemorrhagic strokes; obesity increased the risk of ischemic stroke. Additionally, the positive association of BMI with stroke risk was only observed in participants aged <65 years and was different in men compared to women. In this age group, being overweight increased the risk of both ischemic and hemorrhagic strokes, while being underweight also increased the risk of hemorrhagic stroke, in men. Moreover, in women, being overweight increased the risk of hemorrhagic stroke and being obese increased the risk of total and ischemic strokes.
A meta-analysis involving 2 million participants from 10 countries (including countries in Asia, Europe, and North America) indicated that the relative risks for ischemic stroke were 1.22 for overweight individuals and 1.64 for obese individuals; hemorrhagic stroke was not associated with BMI (27). Previous studies in China showed that the incidences of total and ischemic strokes had a linear relationship with BMI and that there was no significant association between BMI and hemorrhagic stroke (8, 15). In the present study, being overweight or obese (compared to being of a normal weight) were risk factors for developing total and ischemic strokes for the overall population; an increased risk of hemorrhagic stroke was associated with being overweight. Interestingly, previous studies have indicated an increasing prevalence of hypertension, diabetes, and higher BPs in this population over the past decades (18–21, 23). These observations may partly explain the positive association of BMI with the risk of developing stroke in this rural population (28).
Several large prospective studies in eastern Asian individuals, aged <60 years, have failed to identify clear positive associations between the risk of hemorrhagic stroke and a BMI <25 kg/m2 (10, 12, 29). Among individuals with a BMI <25 kg/m2, the mean difference in SBP/DBP was at least 11/5 mmHg compared to normal weight individuals, corresponding to an HR of 1.6 for ICH (30). Further, the risk of hemorrhagic stroke increases with decreasing serum cholesterol levels (31). A study from the United States showed a positive association between elevated BMIs and stroke among individuals aged ≥65 years (32). Higher BMIs also raise the risk of stroke among men aged ≥70 years (33). However, unlike these previous studies, the present study showed that, among men aged <65 years, being overweight was a risk factor for total, ischemic, and hemorrhagic strokes, whereas being underweight was also associated with hemorrhagic stroke. For female participants aged <65 years, being overweight increased the risk of hemorrhagic stroke and being obese increased the risk of ischemic stroke. Among those aged ≥65 years, there were no correlations between BMI and the risk of total, ischemic, or hemorrhagic strokes. The lower prevalence of being overweight or obese among individuals aged ≥65 years compared with those aged <65 years, may have contributed to their lower stroke risk. Further, body fat becomes more likely to be located in the abdominal cavity as age increases; thus, BMI becomes a poorer indicator of overall and abdominal fatness in older individuals (34).
Previous studies in Western countries have shown that BMI is significantly associated with IS among middle-aged men and women (14, 16, 35). However, the association of BMI with hemorrhagic stroke remains controversial. One report showed a linearly opposing correlation (16) whereas others showed no correlation (14, 35). Studies from China indicate that being overweight or obese are risk factors for IS among middle-aged Chinese populations (11, 15); BMI was not associated with hemorrhagic stroke risk in men (15), but was positively correlated with that risk in women (11). Contrary to those observations, our findings indicate that being overweight increases the risk of both ischemic and hemorrhagic stroke and that being underweight also increases the risk of hemorrhagic stroke in men aged <65 years. Moreover, in women, being overweight increased the risk of hemorrhagic stroke and being obese increased the risk of IS. This may be related to the documented association between increased levels of inflammatory markers and the risk of IS (36, 37). Further, obesity is more strongly correlated with elevated high-sensitivity C-reactive protein levels in women than in men (38). Therefore, we hypothesize that metabolic changes related to obesity are more likely to affect the risk of stroke in women than in men. In addition, in the present study, both underweight and overweight individuals were at greater risk of hemorrhagic stroke among men aged <65 years, whereas only being overweight increased the risk of hemorrhagic stroke in women. Ultimately, larger studies are required to clarify the sex-specific effects of BMI on hemorrhagic stroke risk.
It is well known that increased adiposity has adverse effects on insulin sensitivity, lipid metabolism, autonomic tone, fibrinolysis, and inflammation, which contributes to endothelial dysfunction and atherosclerosis (39). In addition, obesity is associated with relatively higher levels of prothrombotic and inflammatory markers (e.g., plasminogen activator inhibitor-1 antigen, fibrinogen, and C-reactive protein) (40, 41), which are associated with IS (36, 42). These may explain the mechanism underlying the association of BMI with developing stroke.
There are several limitations to this study. First, the study population came from a township in northern China that is not representative of the overall national population. However, due to this study being a prospective cohort study in a low-income Chinese population, a larger population study design conducted over a longer period may have reduced the impact of limited representations on the results. Second, the study population was rural Chinese residents with low-incomes and low levels of education and this may limit generalization of the study's findings. However, such rural populations account for more than 50% of China's total population, so our results are representative of this part of the population. Third, the small numbers of patients experiencing stroke during the study periods may have decreased the statistical power to detect possible associations. Fourth, we did not collect all information regarding medicine use for all participants; however, due to their low socioeconomic status, the frequency of medicine use among this population is presumed to be quite low and is not expected to impact the validity of the results. In addition, no patients reported having dyslipidemia at baseline in this study. This may impact the integrated evaluation of the determinants of experiencing stroke. Finally, we only assessed BMI at baseline; central obesity and BMI variation were not addressed in this study. These reduced the power of comprehensively evaluating the association between obesity and stroke risk.
Conclusions
Being overweight increased the risk of both ischemic and hemorrhagic strokes; obesity was only associated with an increased risk of IS. Additionally, the positive association between BMI and stroke risk was only observed in participants aged <65 years and the associations differed between men and women. Being overweight increased the risk of both ischemic and hemorrhagic strokes in men and being underweight increased their risk of hemorrhagic stroke. In women, being overweight increased the hemorrhagic stroke risk, whereas obesity increased their IS risks. The high prevalence of hypertension and elevated BP levels in this low-income population may partially explain the observed positive association between BMI and stroke risk. These findings suggest that weight management should be a high priority for substantially reducing the heavy burden of strokes in rural China, among both men and women aged <65 years; men should maintain their weight within a reasonable range.
Ethics Statement
This study was carried out in accordance with the recommendations of the ethics committee of Tianjin Medical University General Hospital with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
JW, BL, and YL contributed to the conception and design of the work. HG, SS, JL, ZF, YC, JN, CW, and JT contributed the data acquisition. JW and XN contributed the analysis and interpretation of data for the work. HG and SS contributed drafting the work. JW and XN contributed revising the work for important intellectual content. All authors approved of the final version to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the participants of the Tianjin Brain Study and the local medical care professionals for their valuable contributions.
References
1. Chen Z. The Third Nationwide Survey on Causes of Death. Beijing: The Peking Union Medical College Press (2008).
2. Feigin VL, Krishnamurthi RV, Parmar P, Norrving B, Mensah GA, Bennett DA, et al. Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: the GBD 2013 study. Neuroepidemiology. (2015) 45:161–76. doi: 10.1159/000441085
3. Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu S, et al. Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. (2016) 387:251–72. doi: 10.1016/S0140-6736(15)00551-6
4. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2014) 384:766–81. doi: 10.1016/S0140-6736(14)60460-8
5. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of kawasaki disease: a scientific statement for health professionals from the american heart association. Circulation. (2017) 135:e927–99. doi: 10.1161/CIR.0000000000000484
6. Yatsuya H, Toyoshima H, Yamagishi K, Tamakoshi K, Taguri M, Harada A, et al. Body mass index and risk of stroke and myocardial infarction in a relatively lean population: meta-analysis of 16 Japanese cohorts using individual data. Circ Cardiovasc Qual Outcomes. (2010) 3:498–505. doi: 10.1161/CIRCOUTCOMES.109.908517
7. Liu G, Li Y, Hu Y, Zong G, Li S, Rimm EB, et al. Influence of lifestyle on incident cardiovascular disease and mortality in patients with diabetes mellitus. J Am Coll Cardiol. (2018) 71:2867–76. doi: 10.1016/j.jacc.2018.04.027
8. Bazzano LA, Gu D, Whelton MR, Wu X, Chen CS, Duan X, et al. Body mass index and risk of stroke among Chinese men and women. Ann Neurol. (2010) 67:11–20. doi: 10.1002/ana.21950
9. Gajalakshmi V, Lacey B, Kanimozhi V, Sherliker P, Peto R, Lewington S. Body-mass index, blood pressure, and cause-specific mortality in India: a prospective cohort study of 500 810 adults. Lancet Glob Health. (2018) 6: e787–94. doi: 10.1016/S2214-109X(18)30267-5
10. Park JW, Lee SY, Kim SY, Choe H, Jee SH. BMI and stroke risk in Korean women. Obesity. (2008) 16:396–401. doi: 10.1038/oby.2007.67
11. Zhang X, Shu XO, Gao YT, Yang G, Li H, Zheng W. General and abdominal adiposity and risk of stroke in Chinese women. Stroke. (2009) 40:1098–104. doi: 10.1161/STROKEAHA.108.539692
12. Ni MC, Rodgers A, Pan WH, Gu DF, Woodward M. Body mass index and cardiovascular disease in the Asia-Pacific Region: an overview of 33 cohorts involving 310 000 participants. Int J Epidemiol. (2004) 33:751–8. doi: 10.1093/ije/dyh163
13. Saito I, Iso H, Kokubo Y, Inoue M, Tsugane S. Body mass index, weight change and risk of stroke and stroke subtypes: the Japan Public Health Center-based prospective (JPHC) study. Int J Obes. (2011) 35:283–91. doi: 10.1038/ijo.2010.131
14. Jood K, Jern C, Wilhelmsen L, Rosengren A. Body mass index in mid-life is associated with a first stroke in men: a prospective population study over 28 years. Stroke. (2004) 35:2764–9. doi: 10.1161/01.STR.0000147715.58886.ad
15. Wang C, Liu Y, Yang Q, Dai X, Wu S, Wang W, et al. Body mass index and risk of total and type-specific stroke in Chinese adults: results from a longitudinal study in China. Int J Stroke. (2013) 8:245–50. doi: 10.1111/j.1747-4949.2012.00830.x
16. Kroll ME, Green J, Beral V, Sudlow CL, Brown A, Kirichek O, et al. Adiposity and ischemic and hemorrhagic stroke: Prospective study in women and meta-analysis. Neurology. (2016) 87:1473–81. doi: 10.1212/WNL.0000000000003171
17. Feigin VL, Roth GA, Naghavi M, Parmar P, Krishnamurthi R, Chugh S, et al. Global burden of stroke and risk factors in 188 countries, during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. (2016) 15:913–24. doi: 10.1016/S1474-4422(16)30073-4
18. Wang J, An Z, Li B, Yang L, Tu J, Gu H, et al. Increasing stroke incidence and prevalence of risk factors in a low-income Chinese population. Neurology. (2015) 84:374–81. doi: 10.1212/WNL.0000000000001175
19. Ning X, Sun J, Jiang R, Lu H, Bai L, Shi M, et al. Increased stroke burdens among the low-income young and middle aged in rural China. Stroke. (2017) 48:77–83. doi: 10.1161/STROKEAHA.116.014897
20. Wang J, Bai L, Shi M, Yang L, An Z, Li B, et al. Trends in age of first-ever stroke following increased incidence and life expectancy in a low-income chinese population. Stroke. (2016) 47:929–35. doi: 10.1161/STROKEAHA.115.012466
21. Wang J, Ning X, Yang L, Tu J, Gu H, Zhan C, et al. Sex differences in trends of incidence and mortality of first-ever stroke in rural Tianjin, China, from 1992 to 2012. Stroke. (2014) 45:1626–31. doi: 10.1161/STROKEAHA.113.003899
22. The Ministry of Health of the People's Republic of China. The Causes of Death, Disease, and Hurt in Residents. China Health Statistics Yearbook 2011. Beijing: China Union Medical University Press (2011). p. 287–338.
23. Wang J, Ning X, Yang L, Lu H, Tu J, Jin W, et al. Trends of hypertension prevalence, awareness, treatment and control in rural areas of northern China during 1991-2011. J Hum Hypertens. (2014) 28:25–31. doi: 10.1038/jhh.2013.44
24. Disease control Ministry of Health of the People's Republic of China. The Guidelines of Chinese Adult Overweight and Obesity Prevention and Control. Beijing: People's Medical Publishing House (2006). p. 1–3.
25. Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the american heart association/american stroke association stroke council; council on cardiovascular surgery and anesthesia; council on cardiovascular radiology and intervention; council on cardiovascular nursing; and the interdisciplinary council on peripheral vascular disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. (2009) 40:2276–93. doi: 10.1161/STROKEAHA.108.192218
26. Ahmad OB B-PC, Lopez AD, Murray CJL, Lozano R, Inoue M. Age Standardization of Rates: A New Who World Standard. GPE Discussion Paper Series, No 31. Geneva: EIP/GPE/EBD, WHO (2001).
27. Strazzullo P, D'Elia L, Cairella G, Garbagnati F, Cappuccio FP, Scalfi L. Excess body weight and incidence of stroke: meta-analysis of prospective studies with 2 million participants. Stroke. (2010) 41:e418–26. doi: 10.1161/STROKEAHA.109.576967
28. Lu Y, Hajifathalian K, Ezzati M, Woodward M, Rimm EB, Danaei G. Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet. (2014) 383:970–83. doi: 10.1016/S0140-6736(13)61836-X
29. Song YM, Sung J, Davey SG, Ebrahim S. Body mass index and ischemic and hemorrhagic stroke: a prospective study in Korean men. Stroke. (2004) 35:831–6. doi: 10.1161/01.STR.0000119386.22691.1C
30. Chen Z, Iona A, Parish S, Chen Y, Guo Y, Bragg F, et al. Adiposity and risk of ischaemic and haemorrhagic stroke in 0.5 million Chinese men and women: a prospective cohort study. Lancet Glob Health. (2018) 6:e630–40. doi: 10.1016/S2214-109X(18)30216-X
31. Wang X, Dong Y, Qi X, Huang C, Hou L. Cholesterol levels and risk of hemorrhagic stroke: a systematic review and meta-analysis. Stroke. (2013) 44:1833–9. doi: 10.1161/STROKEAHA.113.001326
32. Meschia JF, Bushnell C, Boden-Albala B, Braun LT, Bravata DM, Chaturvedi S, et al. Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2014) 45:3754–832. doi: 10.1161/STR.0000000000000046
33. Dey DK, Rothenberg E, Sundh V, Bosaeus I, Steen B. Waist circumference, body mass index, and risk for stroke in older people: a 15 year longitudinal population study of 70- year-olds. J Am Geriatr Soc. (2002) 50:1510–8. doi: 10.1046/j.1532-5415.2002.50406.x
34. Seidell JC, Visscher TL. Body weight and weight change and their health implications for the elderly. Eur J Clin Nutr. (2000) 54 (Suppl. 3):S33–9. doi: 10.1038/sj.ejcn.1601023
35. Kurth T, Gaziano JM, Rexrode KM, Kase CS, Cook NR, Manson JE, et al. Prospective study of body mass index and risk of stroke in apparently healthy women. Circulation. (2005) 111:1992–8. doi: 10.1161/01.CIR.0000161822.83163.B6
36. Di Napoli M, Papa F, Bocola V. C-reactive protein in ischemic stroke: an independent prognostic factor. Stroke. (2001) 32:917–24. doi: 10.1161/01.STR.32.4.917
37. Rost NS, Wolf PA, Kase CS, Kelly-Hayes M, Silbershatz H, Massaro JM, et al. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: the Framingham study. Stroke. (2001) 32:2575–9. doi: 10.1161/hs1101.098151
38. Saito I, Sato S, Nakamura M, Kokubo Y, Mannami T, Adachi H, et al. A low level of C-reactive protein in Japanese adults and its association with cardiovascular risk factors: the Japan NCVC-Collaborative Inflammation Cohort (JNIC) study. Atherosclerosis. (2007) 194:238–44. doi: 10.1016/j.atherosclerosis.2006.07.032
39. Van Gaal LF, Mertens IL, De Block CE. Mechanisms linking obesity with cardiovascular disease. Nature. (2006) 444:875–80. doi: 10.1038/nature05487
40. Juhan-Vague I, Alessi MC, Morange PE. Hypofibrinolysis and increased PAI-1 are linked to atherothrombosis via insulin resistance and obesity. Ann Med. (2000) 32:78–84.
41. Morange PE, Alessi MC, Verdier M, Casanova D, Magalon G, Juhan-Vague I. PAI-1 produced ex vivo by human adipose tissue is relevant to PAI-1 blood level. Arterioscler Thromb Vasc Biol. (1999) 19:1361–1365. doi: 10.1161/01.ATV.19.5.1361
42. Rost NS, Wolf PA, Kase CS, Kelly-Hayes M, Silbershatz H, Massaro JM, et al. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: the Framingham study. Stroke. (2001) 32:2575–79. doi: 10.1161/hs1101.098151
Keywords: stroke, BMI, subtype, epidemiology, risk factors
Citation: Gu H, Shao S, Liu J, Fan Z, Chen Y, Ni J, Wang C, Tu J, Ning X, Lou Y, Li B and Wang J (2019) Age- and Sex-Associated Impacts of Body Mass Index on Stroke Type Risk: A 27-Year Prospective Cohort Study in a Low-Income Population in China. Front. Neurol. 10:456. doi: 10.3389/fneur.2019.00456
Received: 10 January 2019; Accepted: 15 April 2019;
Published: 01 May 2019.
Edited by:
Linxin Li, University of Oxford, United KingdomReviewed by:
Simona Sacco, University of L'Aquila, ItalyLaurent Puy, Centre Hospitalier Regional et Universitaire de Lille, France
Copyright © 2019 Gu, Shao, Liu, Fan, Chen, Ni, Wang, Tu, Ning, Lou, Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yongzhong Lou, louyongzhong@163.com
Bin Li, libin_1971_2008@sina.com
Jinghua Wang, jhw8799@yahoo.com
†These authors have contributed equally to this work
No comments:
Post a Comment